Read about upcoming changes to UnitedHealthcare coverage.
Where do transplanted organs come from?
Living Donors
Family members or individuals who are unrelated (spouses, friends, co-workers, neighbors, etc.) can donate one of their kidneys to someone who is in need of a kidney transplant.
In some cases, an altruistic donor (a person who wants to donate a kidney but has no specific recipient in mind) may be a donor.
These types of transplants are called living donor transplants. Individuals who donate a kidney can lead healthy lives with the kidney that remains. Visit the Living Donor Kidney Center section of our website to learn more about living donation.
Deceased Donors
Many kidneys that are transplanted come from deceased organ donors. This type of transplant is called a deceased donor (formerly known as cadaveric) transplant.
Deceased organ donors are people who are brain dead and cannot survive their illness and had previously made the decision to donate their organs upon death (by signing up at their local Department of Motor Vehicles or by joining a state or national donor registry). Parents or spouses can also agree to donate a relative's organs. Donors can come from any part of the United States.
There are different types of deceased donors, and it is important to understand the differences between the types because you will need to decide whether or not you are willing to accept a transplant from certain types of donors for your child.
Each donated kidney has a Kidney Donor Profile Index (KDPI) score. This is a score from 0-100 that is calculated based on 10 factors about the donor. The score measures how long the kidney is likely to work. A lower KDPI is better.
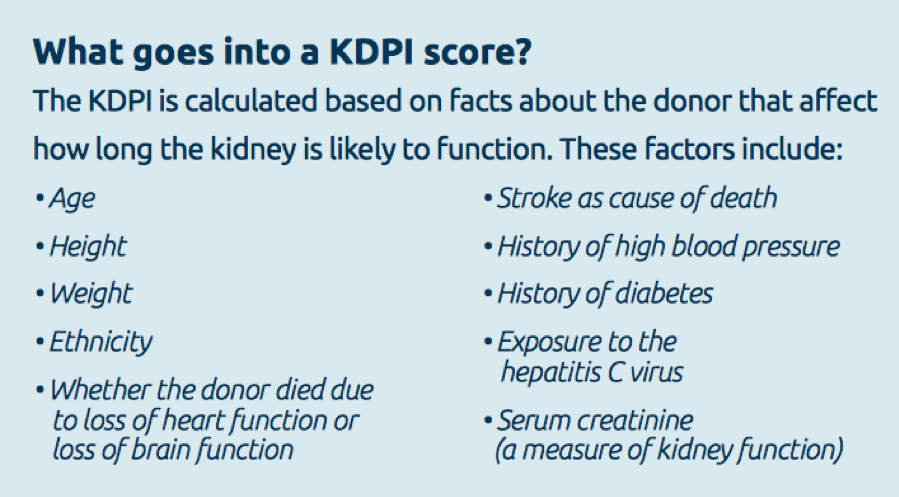
• Low KDPI Score (<20): A low KDPI (under 20) means the kidney is from a donor who was younger and healthier when they died. A kidney with a KDPI score of 20 means it is likely to work longer than most (80%) of other donor kidneys. These kidneys typically last 10-15 years. Patients who receive a low KDPI kidney are usually the youngest and healthiest of the patients on the waiting list (including children), as these patients are expected to need a kidney that has the best capacity to last many years.
• Standard KDPI Score (20 to 85): These kidneys fall between the low and high KDPI kidneys. These kidneys typically last 10 to 15 years. These kidneys are sometimes given to children.
• High KDPI Score (over 85): A high KDPI score (over 85) means the donor was older or sicker when they died. These kidneys typically last 7-10 years after transplant. They are also called ECD (extended donor criteria) kidneys. We do not typically utilize these types of kidneys for children.
PHS Increased Risk Kidneys are another option for patients who want to get transplanted faster. PHS kidneys come from a donor who had a higher chance of having HIV or other blood diseases, such as Hepatitis C due to certain social behaviors (such as intravenous drug use or risky sexual behavior).
These kidneys typically come from younger, healthier donors, and usually last 10 to 15 years. PHS kidneys have a very slightly risk of an infection (less than 0.3%). Learn more about PHS increased risk donors.
When patients do not have any potential living donors, we recommend that patients discuss these special options with their transplant coordinator and physicians, as these kidneys are important opportunities for getting transplanted faster due to the ongoing severe shortage of organs available for transplantation.
How is my child placed on the waiting list for a new kidney?
The first step is to be referred to our transplant center. Your child’s kidney doctor, primary care physician, dialysis unit, or other medical professionals can refer you. In addition, you can contact us to refer your child directly. Your insurance company may also have a list of preferred transplant centers.
Once you are referred to our program, we will ask you some basic questions over the phone and will then schedule you to visit us with your child for a pre-transplant evaluation.
This extensive evaluation must be completed before your child can be placed on the transplant list. Testing includes:
Blood tests are done to gather information that will help determine how urgent it is that your child is placed on the transplant list, as well as ensure that your child receives a donor organ that is a good match. Some of the tests you may already be familiar with, since they evaluate the health of your child’s kidneys and other organs.
These tests may include:
• Blood chemistries — These may include serum creatinine, electrolytes (such as sodium and potassium), cholesterol, and liver function tests.
• Clotting studies, such as prothrombin time (PT) and partial thromboplastin time (PTT) — tests that measure the time it takes for blood to clot.
Other blood tests will help improve the chances that the donor organ will not be rejected. They may include:
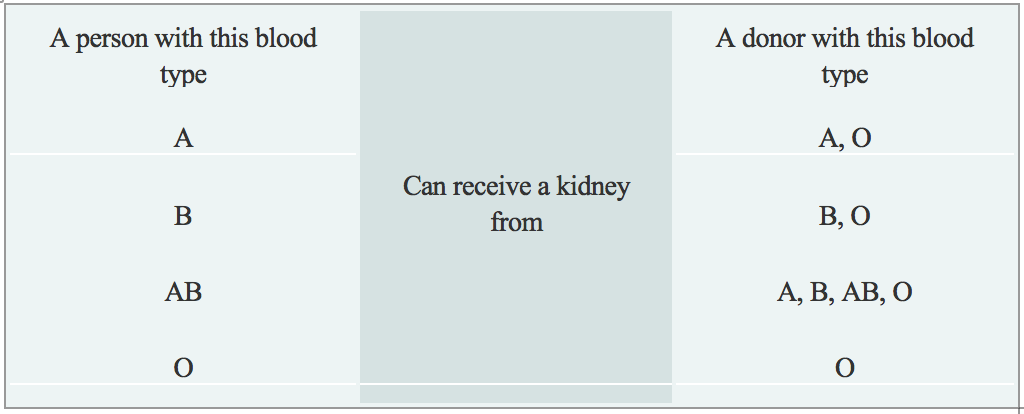
• Blood type: Each person has a specific blood type: type A, B, AB, or O. When receiving a transfusion, the blood received must be a compatible type with your own, or a reaction will occur. A similar reaction will occur if a donor organ of a different blood type is transplanted into your child’s body. These reactions can be avoided by matching the blood types of your child and the donor. The table below describes what blood types are compatible.
• In rare cases, transplants between a donor and recipient who have different blood types may occur by using medications to reduce the chance of a reaction. This is called ABO-incompatible transplantation.
• Human Leukocyte Antigens (HLA) and Panel Reactive Antibody (PRA): These tests help determine the likelihood of success of an organ transplant by checking for antibodies in your child’s blood. Antibodies are made by the body's immune system in reaction to a foreign substance, such as a blood transfusion, a virus, or a transplanted organ, and women may also develop antibodies during pregnancy. Antibodies in the bloodstream will try to attack transplanted organs, therefore, people who receive a transplant must take medications called immunosuppressants that decrease this immune response.
• Viral Studies: These tests determine if your child has been exposed to viruses that may recur after transplant and help us to tailor your child’s medication regimen after transplant.
Diagnostic tests that are performed are necessary to understand your complete medical status. The following are some of the other tests that may be performed, although many of the tests are decided on an individual basis:
• Renal ultrasound: A non-invasive test in which a transducer is passed over the kidney producing sound waves which bounce off of the kidney, transmitting a picture of the organ on a video screen. The test is used to determine the size and shape of the kidney, and to detect a mass, kidney stone, cyst, or other abnormality.
• CT Scan of Abdomen and Pelvis: A diagnostic medical test that produces multiple pictures of the inside of the body. These pictures show your child’s internal organs, bones, soft tissue and blood vessels in greater detail than traditional x-rays. CT scans are used to screen your child for infection, cancer, kidney and bladder stones, abdominal aortic aneurysms (AAA), and to plan for your child’s transplant surgery by seeing their blood vessels in greater detail.
• Kidney biopsy: A procedure in which tissue samples are removed (with a needle or during surgery) from the kidney for examination under a microscope. Biopsies are sometimes used to determine the cause of your child’s kidney disease, which can be important since some kidney disease can recur in the transplanted kidney.
During the evaluation process, you and your child will meet with many members of the transplant team. The transplant team will consider all information from interviews, your child’s medical history, physical examination, and diagnostic tests in determining whether your child can be a candidate for kidney transplantation. After your child’s evaluation is complete and the transplant team believes that your child is an acceptable candidate for transplantation, your child will be placed on the United Network for Organ Sharing (UNOS) waiting list.
![]()
How long will it take to get a new kidney?
There is no definite answer to this question. Sometimes, children wait only a few weeks or months before receiving a donor organ,usually when a living donor is available to donate their kidney.
If your child has a blood type or crossmatch incompatible living donor, you may enter a registry to try to find a suitable match for your child and a suitable recipient for their donor's kidney.
If no living donor is available, it may take years on the waiting list before a suitable donor organ is available. Options such as choosing to accept an increased risk organ may help to reduce your child’s waiting time.
At Weill Cornell Medicine, we are proud that our innovative programs enable us to maximize use of available living and deceased donor organs, giving our patients a shorter waiting time compared to other transplant centers.
While your child is on the waiting list, you will receive close follow-up with your child’s physicians and the transplant team and you and your child will come back for a re-evaluation visit every year. Various support groups are also available to assist you during this waiting time.

Is living donation an option?
We all have heard about the shortage of organs available for transplantation. Unfortunately, the number of deceased donor organs has remained stagnant over the last several years, and this trend is expected to continue. As can be seen from the facts below, there is a great need to increase transplant opportunities for patients with kidney disease.
Although the 16,000+ kidney transplants performed each year in the United States may sound like a lot, the number is small compared to the number of people who are on dialysis, which is more than 650,000. It is also quite small when compared to the number of people waiting for a kidney (more than 95,000) and those never even referred for transplant evaluation (130,000+).
Given the high rate of complications and death while on dialysis, an increase in living donor kidney transplants holds the hope for improving the ability to transplant people who need a kidney.
Benefits of Living Donor Over Deceased Donor Kidney Transplantation
In addition to increasing the number of kidney transplants, living donation also provides the following benefits:
• Ability to schedule the transplant at a time that is convenient for both the donor and recipient helps to facilitate pre-emptive transplantation (transplant before the recipient needs dialysis), which is associated with better outcomes for the recipient
• Superior quality of living donor organs (as compared to deceased donor organs) leads to:
• Better function of the transplanted organ (immediate in the overwhelming majority of cases)
• Longer survival of the transplanted organ

What can I expect when my child gets a kidney transplant?
If all goes well and your child is designated to receive the kidney transplant, the surgery takes about 2 to 4 hours.

For pediatric patients with complex genitourinary anatomy, the surgery may take longer if the child requires urologic surgery at the same time as their transplant.
In most cases, the diseased kidneys are left in place during the transplant procedure, although some children require removal of one or both of their native kidneys at the same time as their transplant. The transplanted kidney is placed in the lower abdomen on the front side of the body.
Read more about the kidneys and how they work.
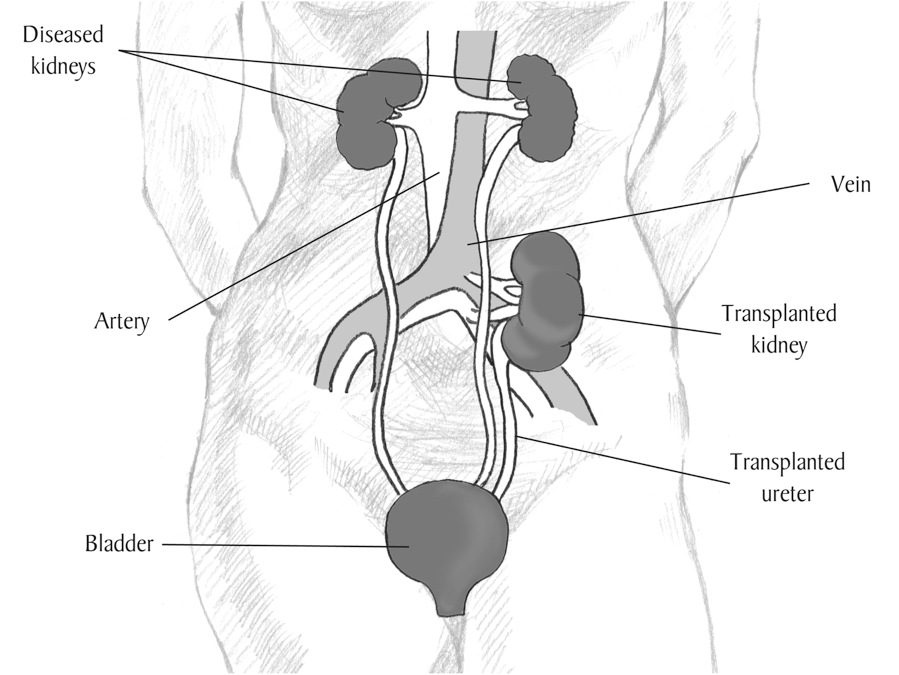
Image courtesy of the National Institute of Diabetes and Digestive and Kidney Diseases, National Institutes of Health
The transplant is performed under general anesthesia, and after the surgery, your child will be transferred to the Pediatric Intensive Care Unit (ICU) for close monitoring.
Most children remain in the hospital for 4 to 7 days after their kidney transplant. Your child’s recovery period will consist of having his/her diet advanced, getting out of bed to walk, and participating in educational sessions with nurses, pharmacists, nutritionists, social workers, and others.
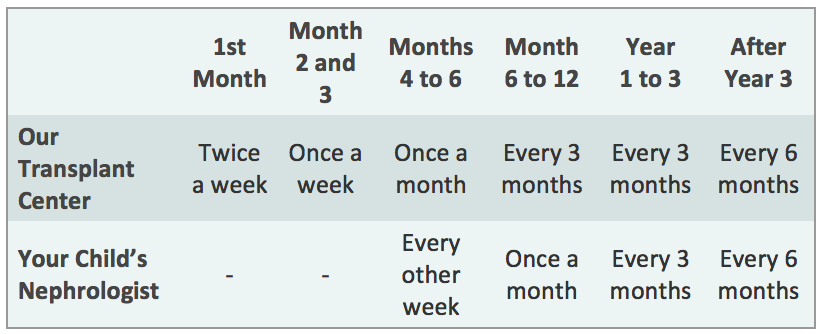
After your child is discharged from the hospital, you should expect to come back to the transplant clinic 2 to 3 times a week for the first month, then weekly for the next two months, then less frequently, depending on how your child is doing.
Your child will also be able to return to the kidney doctor who was caring for them before their transplant. We will work closely with your child’s doctor to manage their transplant, and you will continue to visit our Transplant Center periodically to ensure that your child’s kidney is functioning well, according to the schedule below. However, more frequent visits to the transplant center may be needed depending on your child’s post-transplant course.
What is done to prevent rejection?
Medications must be given for the rest of the life of your child’s transplant kidney to fight rejection. Each person is individual, and the transplant team customizes your medication regimen to your child’s specific needs.
The anti-rejection medications most commonly used include:
Intravenous medications given in the hospital at the time of transplant:
• Rabbit anti-thymocyte globulin (Thymoglobulin) or
• Basiliximab (Simulect)
Oral medications taken for as long as transplant continues to function:
• Tacrolimus (Prograf or Advagraf or Envarsus XR) and
• Mycophenolate mofetil (CellCept)or mycophenolate sodium (myfortic)
Some patients may also receive one or more of the following medications, usually when they are at higher risk for rejection due to prior transplants, prior blood transfusions, and/or pregnancy:
• Prednisone
• Rituximab (Rituxan)
• Intravenous immune globulin (IVIG)
Usually, several anti-rejection medications are given initially. The doses of these medications may change frequently as your child’s response to them changes.
Because anti-rejection medications affect the immune system, people who receive a transplant will be at higher risk for infection. A balance must be maintained between preventing rejection and making your child susceptible to infection.
Blood tests to measure the amount of medication in the body are done at follow-up visits to make sure you do not get too much or too little of the medications.

This risk of infection may be higher in the first few months after transplant because higher doses of anti-rejection medications are given during this time. However, in the first few months after your child’s transplant, they will be given several medications to reduce the risk of certain types of infection.
