Read about upcoming changes to UnitedHealthcare coverage.
How am I placed on the waiting list for a new pancreas?
The first step is to be referred to our transplant center. Your diabetes doctor (endocrinologist), primary care physician, dialysis unit (if you also have kidney failure), or other medical professional can refer you. In addition, you can contact us to refer yourself directly. Your insurance company may also have a list of preferred transplant centers.
Once you are referred to our program, we will ask you some basic questions over the phone and will then schedule you to visit us for a pre-transplant evaluation. This extensive evaluation must be completed before you can be placed on the transplant list. Testing includes:
• Blood tests
• Diagnostic tests
• Psychological/social evaluation
Blood tests are done to gather information that will help determine how urgent it is that you are placed on the transplant list, as well as ensure that you receive a donor organ that is a good match. Some of the tests you may already be familiar with, since they evaluate your general health and organ function. These tests may include:
• Blood chemistries — these may include glucose, serum creatinine, electrolytes (such as sodium and potassium), cholesterol, and liver function tests.
• Clotting studies, such as prothrombin time (PT) and partial thromboplastin time (PTT) - tests that measure the time it takes for blood to clot.
• Diabetes-related tests, such as hemoglobin A1c, c-peptide levels, and antibody levels related to the diabetes autoimmune process
Other blood tests will help improve the chances that the donor organ will not be rejected. They may include:
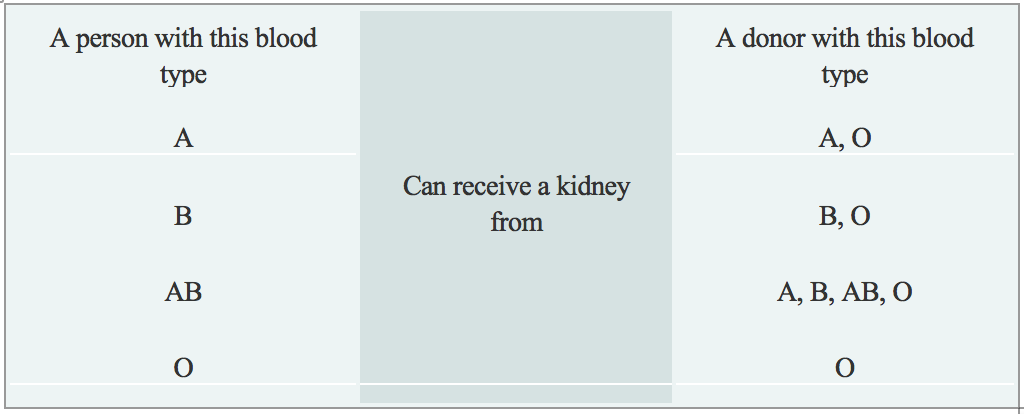
• Blood type: Each person has a specific blood type: type A, B, AB, or O. When receiving a transfusion, the blood received must be a compatible type with your own, or a reaction will occur. A similar reaction will occur if a donor organ of a different blood type is transplanted into your body. These reactions can be avoided by matching the blood types of you and the donor. The table below describes what blood types are compatible.
• Human Leukocyte Antigens (HLA) and Panel Reactive Antibody (PRA): These tests help determine the likelihood of success of an organ transplant by checking for antibodies in your blood. Antibodies are made by the body's immune system in reaction to a foreign substance, such as a blood transfusion, a virus, or a transplanted organ, and women may also develop antibodies during pregnancy. Antibodies in the bloodstream will try to attack transplanted organs, therefore, people who receive a transplant must take medications called immunosuppressants that decrease this immune response.
• Viral Studies: These tests determine if you have been exposed to viruses that may recur after transplant, and help us to tailor your medication regimen after transplant.
Diagnostic tests that are performed are necessary to understand your complete medical status. The following are some of the other tests that may be performed (if you also require a kidney transplant), although many of the tests are decided on an individual basis:
• Renal ultrasound: A non-invasive test in which a transducer is passed over the kidney producing sound waves which bounce off of the kidney, transmitting a picture of the organ on a video screen. The test is used to determine the size and shape of the kidney, and to detect a mass, kidney stone, cyst, or other abnormality.
• CT Scan of Abdomen and Pelvis: A diagnostic medical test thatproduces multiple pictures of the inside of the body. These pictures show your internal organs, bones, soft tissue and blood vessels in greater detail than traditional x-rays. CT scans are used to screen you for infection, cancer, kidney and bladder stones, abdominal aortic aneurysms (AAA), and to plan for your transplant surgery by seeing your blood vessels in greater detail.
During the evaluation process, you will meet with many members of the transplant team. The transplant team will consider all information from interviews, your medical history, physical examination, and diagnostic tests in determining whether you can be a candidate for pancreas transplantation. After your evaluation is complete and the transplant team has determined that you are a suitable candidate for a pancreas transplant, you will be placed on the United Network for Organ Sharing (UNOS) waiting list.
What can I expect when I get a pancreas transplant?
If all goes well and you are designated to receive the pancreas transplant, the surgery takes about 3 to 5 hours. It is performed under general anesthesia, and you will spend several days in the surgical intensive care unit after the surgery so that you and the function of the new pancreas can be closely monitored.
Check out the various steps of the pancreas transplant procedure by clicking here.
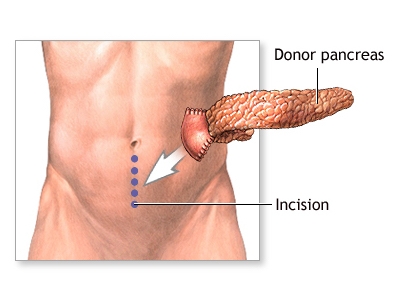
The majority of pancreas transplant recipients will have a nasogastric tube (a tube placed during surgery) that prevents too much pressure from building up in the intestines where the new pancreas is connected. Because of this, it will be several days before you are able to eat, and the majority of your medications will be given through your intravenous line (tube placed in your vein).
If you are doing well, you will be transferred to the Transplant Unit within several days of your surgery, and will likely be in the hospital for a total of six to eight days. Once on the transplant unit, you will begin your recovery period that includes having your diet advanced, getting out of bed to walk, and participating in educational sessions with nurses, pharmacists, nutritionists, social workers, and others.
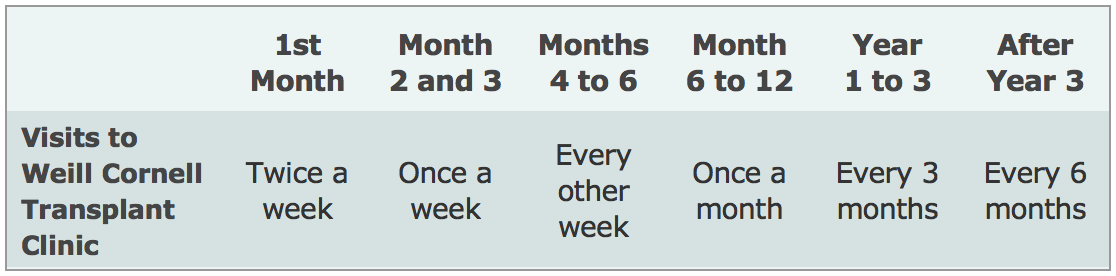
After you are discharged from the hospital, you should expect to come back to the transplant clinic two to three times a week for the first month, then weekly for the next two months, then less frequently, depending on how you are doing.
You will also be able to return to the doctor(s) who was caring for you before our transplant, such as your endocrinologist. We will work closely with your doctor to manage your transplant, and you will continue to visit our Transplant Center periodically to ensure that your pancreas is functioning well, according to the schedule below. However, more frequent visits to the transplant center may be needed depending on your post-transplant course or if you choose to participate in a research study.