Read about upcoming changes to UnitedHealthcare coverage.
Whether you see us in-person or by Video Visit, we're here for you. See how we're keeping you safe.
"Paresis" means partial paralysis. Vocal fold paresis refers to a vocal fold with motion impaired (but not absent – that condition is called vocal fold paralysis) because the nerve in the muscles of the vocal fold is damaged. Most commonly, this happens as a result of a routine viral infection like a cold, although any surgery that can cause vocal fold paralysis can also cause paresis. Paresis is generally not caused by tumors pressing on the nerve, although there may be very rare exceptions.
Problems result because even though the vocal fold can move, it cannot meet the other vocal fold to close well during voicing. Or, it can meet the other vocal fold, but only with unusual or extreme effort.
Because the vocal folds cannot close well during voicing, the voice may be soft, hoarse or breathy. As the closure is not severely compromised, changes can be very subtle or apparent only in challenging acoustic situations, such as when speaking over background noise, teaching class, or giving a presentation. An individual with paresis may be aware of an unusual amount of effort, or a sense of breathlessness, during prolonged or loud talking. Sometimes, muscles not usually involved in voicing will be engaged to try to bring the vocal folds together, which can cause pain when speaking. Occasionally, there may be no evident voice change at all, and pain and/or breathlessness when speaking may be the only signs of the problem. Paresis is usually relatively prompt in onset, so individuals are able to recall a fairly precise time that their voice changed.
Vocal fold paresis is one of the most challenging diagnoses is laryngology because the changes from normality are often slight. In general, a physician looks for limitations in motion of one vocal fold, and signs of impaired closure. There may be thinning of the affected vocal fold or atrophy of muscle mass. In addition, the other vocal fold may show signs of unusual muscular effort during voicing.
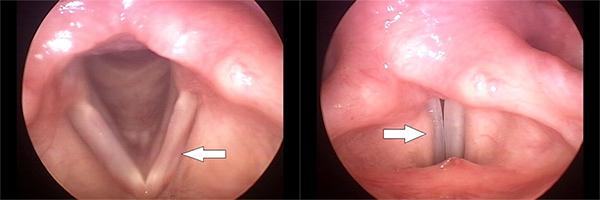
At left, the vocal folds are shown during quiet breathing. The arrow shows thinning of the left vocal fold, indicative of paresis on that side. At right, the vocal folds are shown during voicing. The arrow indicates the bulge of the ventricular fold on the good side, suggesting unusual muscular effort being used to bring the folds together. Note that the gap between the vocal folds is not obvious.
The greatest challenge in the diagnosis of vocal fold paresis may be distinguishing it from insignificant asymmetries of motion of the two vocal folds. There is no biological requirement for the vocal folds to move in perfect coordination, and laryngeal asymmetries are routine findings in patients evaluated for unrelated complaints. If one is so inclined, one could find signs suggesting paresis in virtually every adult or, at the other extreme, one could dismiss every asymmetry as meaningless. Clinical judgment is necessary to separate paresis from innocent motion abnormalities – signs should be consistent with one another and match the patient’s symptoms as well as the history of the complaint.
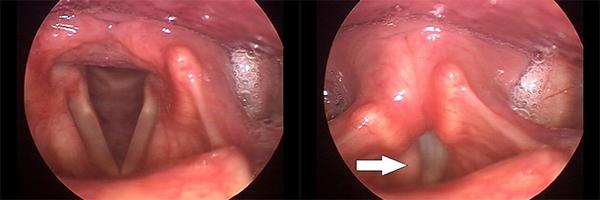
In another case, there is no obvious asymmetry between the vocal folds during quiet breathing, at left. During voicing however, the extreme effort exerted by the unaffected right vocal fold is apparent (arrow).
Some cases of vocal fold paresis recover by themselves over several weeks or months. Neither resting the voice nor exercising the vocal folds has been shown to have any effect on recovery. Similarly, no medicine has been proven to help.
Some physicians have found a test known as electromyography (EMG) to be helpful in diagnosing paresis. EMG is performed by putting needles into the muscles of the larynx through the skin of the neck for a few minutes to record electrical activity. However, there is debate about whether EMG is sensitive enough to correctly identify mild paresis, and/or if every mild abnormality identified by EMG signifies paresis.
Because both voice problems and the gap between the vocal folds resulting from paresis are relatively mild, voice therapy is a reasonable initial treatment. By itself, it may be sufficient to overcome the limitations of paresis, and may help minimize any muscular discomfort. Should the paresis not recover and should voice therapy be insufficient to address the resulting problems, it is possible to address voice quality and other symptoms by repositioning the weak vocal fold closer to its partner. This is known as medialization. In brief, this can be accomplished by injecting the vocal fold with one of a number of available substances (injection augmentation), or by placing a block of artificial material into the larynx through an operation on the outside of the neck (medialization laryngoplasty). Each technique has its own advantages, and making an intelligent choice among available treatments depends upon detailed discussion with your physician.