Read about upcoming changes to UnitedHealthcare coverage.
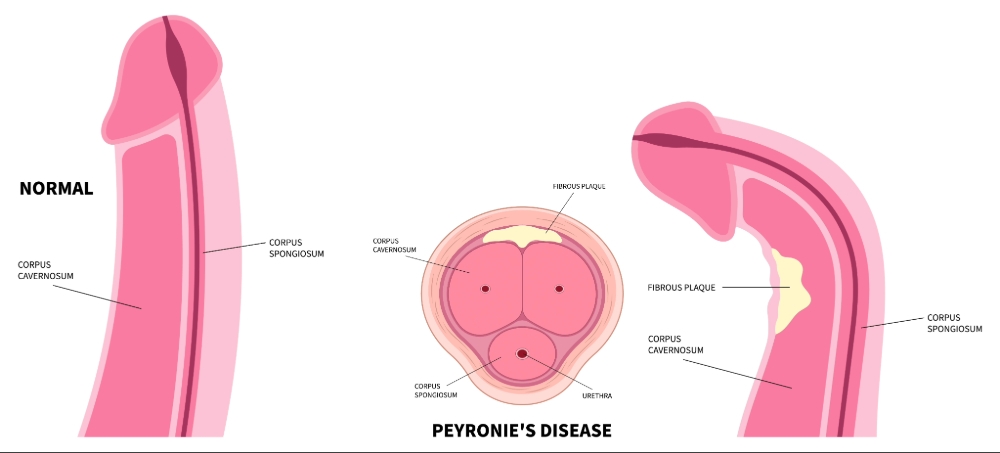
Peyronie's disease is a medical condition characterized by the development of a lump on the shaft of the penis. This lump is a scar (plaque) that forms on the lining (tunica albuginea) of the penile erectile body (corpus cavernosum). It is believed to be the result of direct injury to the penis. Early on following the trauma, an inflammatory reaction occurs, often bringing a man's attention to the problem because of pain associated with his erection. With time, the inflammation progresses and a scar develops. The time to develop this scar and the degree to which it occurs varies from patient to patient. Often the process heals itself over the first 12 months. In some cases, however, the scar formation is severe. In these cases, the scar becomes progressively harder and more obvious, causing the penis to curve during erection. While the scar is benign (non-cancerous), the resulting curvature may lead to the inability to have sexual intercourse. This may also interfere with ones ability to get and maintain an erection.
Originally, the incidence of Peyronie's disease was estimated to be approximately 1-3%. More recent research suggests that the incidence is far higher, at approximately 8.9%. This same research estimates that roughly one third of patients do not even know they have this condition.
Peyronie's disease is characterized by a localized scarring of the tunica albuginea of the penis. The cause of Peyronie's disease appears to be multi-factorial and has not been fully explained. As bending of the penis occurs in all men during penetrative sexual intercourse, only a small percentage of men manifest plaque formation. While trauma is believed to be the initial event, many theories have been proposed for the pathogenesis of Peyronie's disease, including auto-immune factors, excess production of chemicals (known as cytokines) in the tissue of the penis and abnormalities of cell behavior. Peyronie's disease appears to be more common in certain ethnic groups, particularly northern European Caucasians; it is uncommon in African-American men and rare in Asian men.
Risks of Peyronie's Disease include advanced age, diabetes and erectile dysfunction. It is also believed that there is an association between Peyronie's disease and Dupuytren's disease (aka Dupuytren's contracture). Dupuytren's disease is a scarring (fibromatosis) of the hand leading to hand deformities. Between 10-20% of men with Peyronie's disease will also have Dupuytren's disease. Having prostate cancer surgery is also a risk factor for developing Peyronie's disease. As many as 16% of men undergoing surgery for prostate cancer may develop Peyronie's disease within 3 years of having surgery. Another possible cause of Peyronie's disease was believed to be hypogonadism, or low testosterone, although this has not held true.
Men with Peyronie's disease typically present to a physician in a number of ways, including painful erections, penile curvature or erectile dysfunction (ED).
The degree of these symptoms can vary significantly between patients and even among the same patient over time. It is not uncommon for patients to delay evaluation and treatment for up to one year. This can be due to a high degree of patient embarrassment and social stigma. It is also very common for males with Peyronie's disease to experience a loss of sexual self-confidence, attractiveness and psychological distress.
Peyronie's disease can be classified into two phases: the acute (early, active) phase and the chronic (late, stable) phase. The acute phase can last up to 18 months, but is often much shorter. It is characterized by an evolving change in plaque consistency and penile deformity. The chronic phase immediately follows the acute phase and is characterized by resolution of pain and curvature stabilization.
It is estimated that approximately 12% of men who have Peyronie's disease will have improvement or complete correction of their penile curvature within the first 12 months of their condition. Thus, as the plaque in Peyronie's disease may shrink or disappear without treatment, medical experts suggest waiting a full year before attempting to correct it surgically. It is during the acute phase that patients often seek counseling and treatment, although no treatment has been proven to be of significant benefit during this period.
When evaluating a patient with Peyronie's disease it is important to examine the penis in its entirety. Feeling for the location, size and consistency of the plaque (or plaques) is of utmost importance. If possible, examining the penis in the erect state is ideal because it affords the ability to measure the angle of curvature, location of maximal curvature, and presence of any indentation deformities (known as an hourglass deformity).
While some men may improve their curvature spontaneously, many men will progress over the first 12 months. Some men may have a persistent and complete inability to achieve penetration because of either the magnitude of the penile curvature or erectile dysfunction (ED). Treatment options largely depend on the severity of penile curvature and erectile dysfunction. All patients considered candidates for surgical correction should undergo penile vascular evaluation. Doing this allows the clinician to predict which patients may have worsening of their erectile function following penile reconstruction. In part, the operative intervention that is selected for the individual patient is based upon their preoperative erectile function.
There is no uniformly agreed upon treatment algorithm for males in the acute phase of Peyronie's disease. Similarly, there is a lack of strong evidence supporting oral medication in the treatment of Peyronie's disease. Experts in sexual medicine often prescribe oral medications during the acute phase of Peyronie's disease in hopes of mitigating worsening penile scarring. This practice is often specialist dependent. Penile traction is occasionally used in the acute and chronic phase. The belief is that stretching of the penis facilitates improvement of the penile curvature and decreases penile length loss. Only a few studies have demonstrated this to be true.
Intralesional (into the plaque) injection of medication is another treatment option for males with Peyronie's disease. Currently, collagenase Clostridium histolyticum (Xiaflex®) is the only FDA approved pharmacologic treatment of Peyronie's disease. It is administered as an intralesional injection in a series of 1-4 cycles every 6 weeks. This has been shown to result in a 32-34% decrease in penile curvature. Adverse events are common and include penile pain, bruising and swelling. There is also a risk of of penile fracture, although this is less than 1%. Other intralesional medications are also used in the acute and chronic phase of Peyronie's disease. These medications include verapamil and interferon.
Patients who fail to respond to drug therapy for Peyronie's disease and who have curvature for longer than 12 months are considered candidates for surgical intervention. Which corrective operation is chosen is based on a number of criteria which include:
There are 3 major types of operations for Peyronie's disease.
This group of procedures generally involves performing a tuck procedure on the side opposite to the scar (plaque). Its advantages include its simplicity, excellent preservation of preoperative erection ability and high patient satisfaction. The disadvantages include loss of penile length, which in the medical literature is reported to occur in 46-100% of patients. Patients who are considered excellent candidates for this procedure include those with ample penile length who have a simple curvature without any other associated deformity (i.e., hour-glass).
This group of procedures involves the complete or partial excision of the plaque or its incision with the placement of a graft into the space left by the excision/incision technique. Multiple graft materials have been used, including dermis, cadaveric fascia, cadaveric pericardium, saphenous vein and intestinal submucosa. The advantage of this approach is that it is typically not associated with loss of penile length. Its disadvantages include the development of postoperative erectile dysfunction in men with poor erectile function preoperatively and prolonged loss of penile sensation in approximately 10% of men. Ideal candidates for this approach are men with complex penile curvatures who have normal erectile function preoperatively. Men who present with hour-glass deformity are also best served by plaque incision and grafting.
The placement of a penile implant allows immediate correction of the penile curvature as well as permitting fully rigid erections. It is associated with excellent postoperative patient satisfaction rates. It is reserved for men with combined erectile dysfunction and penile curvature.
To request an appointment, please call our office at (646) 962-9600. Our phone staff are available to help you Monday-Friday, from 9AM-5PM (EST).
If you'd like to learn more about our providers that specialize in Peyronie's Disease, please view the "Our Care Team" page.