The detection of adrenal masses has increased with the widespread use of high resolution imaging techniques such as Computed Tomography (CT or CAT scan) and Magnetic Resonance Imaging (MRI) scan.
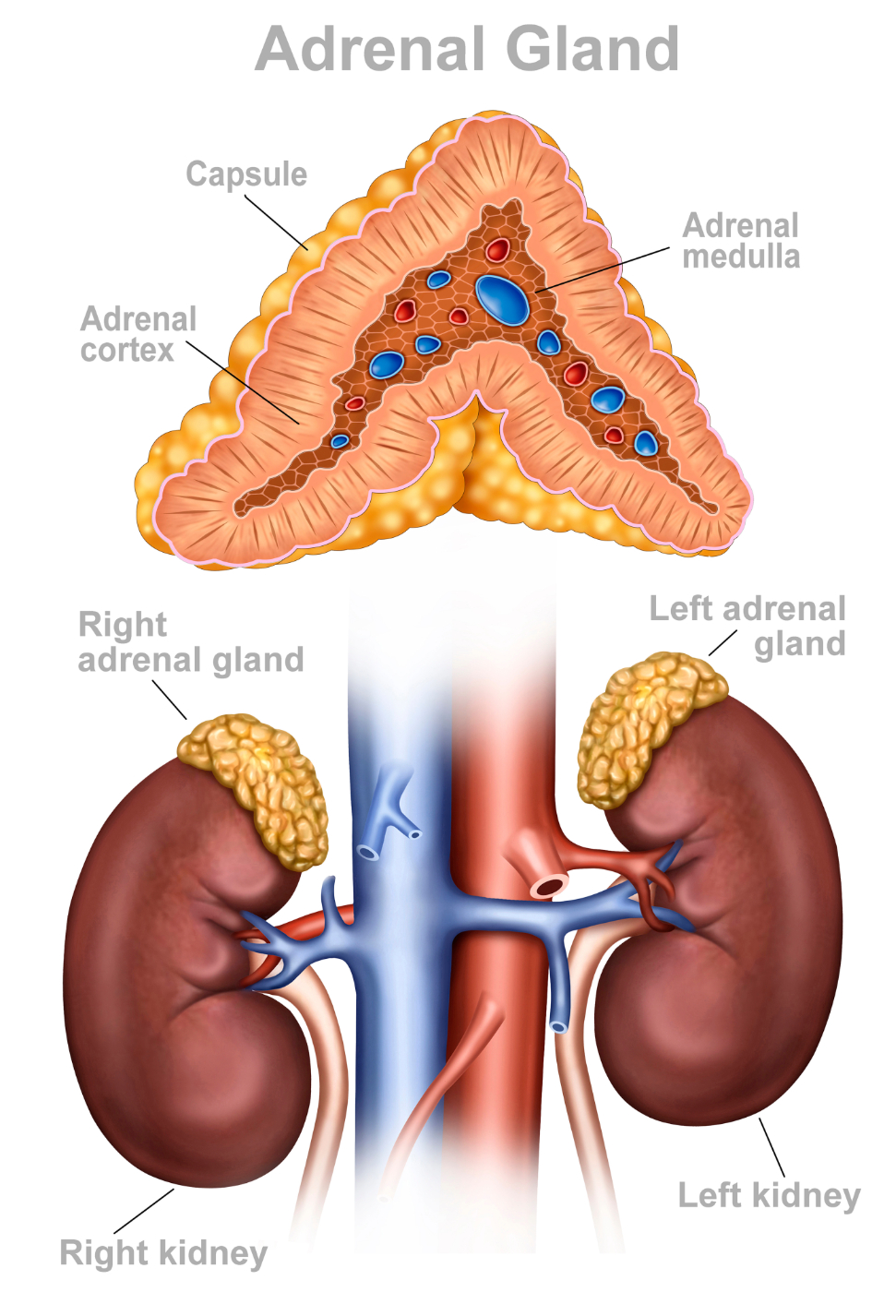
The adrenal glands are paired structures located in the back of the abdomen, just above the kidneys.The adrenal glands produce steroid and other hormones that help regulate blood pressure, kidney function, responses to stress, and some sexual functions.Therefore, the approach to the evaluation of most adrenal masses depends upon the radiographic appearance of the lesion, whether the patient has any symptoms from overproduction of one of the adrenal hormones, and whether the patient has a known primary malignancy.
The two parts of the adrenal glands, the adrenal cortex and adrenal medulla, perform separate functions and produce separate hormones.
- The adrenal cortex produces glucocorticoids (cortisol), mineralocorticoids (aldosterone), and androgens (sex hormones). Cortisol has important effects on heart, blood pressure, metabolism and your immune system. Aldosterone is necessary for fluid and electrolyte balance, which affects your blood pressure. The adrenal androgen hormones regulate sexual characteristics.
- The adrenal medulla is responsible for producing epinephrine and norepinephrine (adrenaline), with effects on blood pressure and bodily stress responses. Both deficiency and overproduction of these hormones can cause significant problems. Overproduction of these hormones may be due to a tumor of the adrenal gland, which is an indication for your doctor to send you for a urologic consultation.
Most adrenal lesions represent benign nonfunctioning masses called adenomas. The vast majority are discovered during an examination that is being performed for reasons other than suspected adrenal disease. In some cases, they represent benign lesions that may secrete hormones that can affect blood pressure or steroid/sugar levels. In other cases, these adrenal lesions can represent a metastatic lesion in a patient with a known primary malignant lesion.
Benign Lesions of the Adrenal Glands - Symptoms & Evaluation
Incidental Tumor:
Most adrenal tumors do not produce hormones (non-functional) and are found incidentally on CT or MR imaging, therefore not causing symptoms. An adrenal incidentaloma is found in up to 5% of all people who are undergoing imaging studies for another medical condition. A history and physical examination for symptoms and signs of excessive hormonal production, and order blood and urine tests to rule out overproduction of hormones by the incidentaloma, will be carried out.
Adrenal Cushing's Syndrome:
In adrenal Cushing's syndrome, excess cortisol is produced by adrenal gland tumors or hyperplastic adrenal glands.
Signs/Symptoms:
- Weight gain and fat distribution mostly in the abdominal region
- Easy bruising/thinning of the skin
- Poor wound healing
- Round face
- Weak bones, which can lead to fractures
- Fatigue
- High blood pressure
- High blood sugar
- Irritability, anxiety, mood swings and/or depression
- Increased acne
- Increased thirst and urination
- Lack of menstrual periods/excessive facial hair in women
Evaulation:
- Review of all the medicines you are now taking; taking steroids for another medical condition such as arthritis, asthma, inflammatory diseases, and organ transplantation can cause Cushing's syndrome
- 24-hour urine evaluation
- Blood tests
- Radiographic tests such as CT or MR imaging to look for tumors on the adrenal or pituitary glands
Primary Hyperaldosteronism/Conn's Syndrome:
Conn's Syndrome occurs with the overproduction of the hormone aldosterone by the adrenal glands.
Common signs/symptoms:
- Most patients have no complaints, but have high blood pressure that does not respond to conventional treatment.
- Low potassium is diagnosed on routine blood tests
Other symptoms/signs may include:
- Headaches
- Excessive urination and thirst
- Muscle weakness or cramps
- Evaluation of Hyperaldosteronism
Evaulation:
- Blood tests to check potassium, aldosterone, and renin levels
- 24-hour urine examination
- Radiographic tests such as CT or MR imaging to look for tumor on the adrenal gland
- If the CT or MR images do not show a tumor because of its small size, but excessive aldosterone is being produced, you may have another test performed called adrenal venous sampling, where a radiologist will obtain blood samples directly from each adrenal gland to determine which adrenal gland (right or left) is the cause.
Pheochromocytoma:
Pheochromocytomas are tumors that cause overproduction of cathecholamine hormones, such as epinephrine and norepinephrine, that are involved in maintaining blood pressure. Excessive secretion of these hormones can cause very high blood pressure, heart palpitations, anxiety and sweating. Though a rare cause of high blood pressure, if left untreated, they can cause serious consequences, including heart attack, stroke, and arrthymia.
In most cases, a pheochromocytoma is a single, benign tumor that sporadically occurs in a patient without a family history of hormonal or endocrine problems. However, a small percentage may be linked to hereditary causes.
Signs/symptoms:
Episodes of high blood pressure with associated:
- Sweating
- Headache
- Heart palpitations
- Anxiety
These may be brought on by exercise, emotional stress, or anesthesia, as well as increases in abdominal pressure during urination or defecation.
Evaluation:
- Blood tests to check cathecolamine levels
- 24-hour urine examination to assess levels of these hormones in your urine
- You will likely be asked to abstain from alcohol and caffeine intake 24 hours prior to the examinations
- Radiographic tests such as CT or MR imaging to look for tumor on the adrenal gland
Metastasis of Primary Malignancy to the Adrenal Gland:
Although most adrenal lesions are benign non-functional adenomas, masses in patients with a known primary extra-adrenal malignancy require evaluation. The most common primary malignancies with adrenal metastases are carcinomas of the lung, breast, and melanoma. In general, metastatic lesions can be larger than benign adrenal adenomas and appear more heterogeneous and irregular on CT or MR imaging. In some cases, percutaneous biopsy may be recommended for definitive diagnosis.
Benign Lesions of the Adrenal Glands - Treatment Options
Adrenal Incidentaloma Treatment:
Management of an incidentally found adrenal mass in a patient without a known primary malignancy will depend upon the size of the mass, its characteristics on the CT or MRI scan, and whether hormonal tests indicate that the tumor is producing excessive adrenal hormones.
The two options for treating adrenal incidentaloma are:
Monitoring its appearance with a series of CT or MRI scans
Removing the adrenal mass with minimally invasive surgery, usually laparoscopically. It typically involves removal of the mass and the adrenal gland (adrenalectomy). In select cases, removal of only the tumor may be recommended (partial adrenalectomy). This surgery may be done through a single small incision in the abdomen (Single Site laparoscopic surgery) or through 3-4 small keyhole incisions. Robotic surgery may also be recommended by your surgeon. If the lesion is large and/or looks suspicious on the CT or MR imaging, the mass is secreting excessive adrenal hormones. Surgery recovery will typically require a 1-2 day hospitalization and 10-14 day recovery period.
Adrenal Cushing's Syndrome Treatment:
Treatment of adrenal tumors that cause Cushing's syndrome include laparoscopic surgery and possible medication to reduce the production of cortisol.
Hyperaldosteronism/Conn's Syndrome Treatment:
Treatment of an aldosterone producing tumor involves monitoring and replacing serum potassium levels and laparoscopic adrenal removal or partial adrenalectomy. Along with recovery from surgery, you will see your primary doctor for blood pressure and serum potassium monitoring. Your blood pressure may normalize or you may require blood pressure medication after surgery.
Adrenal Pheochromocytoma Treatment:
The preferred treatment for adrenal pheochromocytoma is surgical removal of the functional adrenal tumors. Most cases are done through minimally invasive approaches. Medical treatment is a crucial part of treatment prior to the adrenal surgery in order to suppress effects of the excessive hormone secretion.
Metastasis of Primary Malignancy to the Adrenal Gland Treatment:
The treatment of metastatic lesions of the adrenal gland depend upon the primary malignancy. Management is usually dictated by the physician treating the primary malignancy. It may center upon medical management with chemotherapy or other medications or possible surgical excision.
Would you like an appointment?
Please call our office at (646) 962-9600 to schedule an appointment via phone. Our phone staff are available to help you Monday-Friday, from 9AM-5PM (EST).
If you'd like to learn more about each of our providers that specialize in Benign Lesions of the Adrenal Gland, please view the "Our Care Team" page.