Read about upcoming changes to UnitedHealthcare coverage.
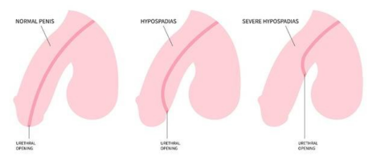
Hypospadias is a condition where the hole in the penis is not at the tip of the penis, but rather somewhere on the underside of the shaft or scrotum. It is typically associated with an incomplete foreskin and a downward curvature of the penis (chordee).
Hypospadias is typically classified based on the location of the opening on the opening.
It is not known exactly why hypospadias occurs. There are theories that certain environmental and hormonal exposures during pregnancy may be associated with hypospadias. There can also be a genetic component to hypospadias.
Hypospadias is usually diagnosed when a child is born. At this time, if circumcision is considered for the baby, it is important to delay this procedure until the child is seen by a urologist as the foreskin can provide skin that is needed to reconstruct the urethra.
Ultimately, hypospadias is repaired through surgery under general anesthesia. Typically, the repair is done between ages 6 – 18 months of age. The correction involves straightening the penis, bringing the opening to the normal location and giving the penis a circumcised appearance. Typically the child will require a stent or catheter to remain in place for up to a week to allow for drainage during healing. Treatment is highly individualized, and the techniques vary considerably based on each child’s anatomy.
In severe or complicated cases, particularly those with severe curvatures, the surgery is often done in 2 or 3 stages, each scheduled 6 months apart. In some cases, grafts from the inner lip or cheek must be taken from other parts of the body and used in the repair. Select patients may be recommended to start testosterone therapy prior to surgery, and occasionally, hyperbaric oxygen therapy will be used to supplement healing.
The Division of Pediatric Urology at Weill Cornell Medicine, proudly affiliated with Children’s Hospital of New York at NewYork-Presbyterian, provides world-class care to children of all ages, from birth through adolescence, with disorders of the kidney, ureter, bladder, urethral and external genitalia. Our board-certified and fellowship-trained pediatric urologists offer minimally invasive robotic and laparoscopic procedures, complex open procedures and non-surgical management of pediatric urological disorders. Our program is a top Pediatric Urology program in New York City, and NewYork-Presbyterian Children’s Hospital-Columbia and Cornell is ranked among the top 50 pediatric urology programs in the United States by U.S. News & World Report.
To request an appointment, please call our office at (212) 746-5337 or schedule an appointment with one of our providers online below. Our phone staff are available to help you Monday-Friday, from 9AM-5PM (EST).
Meet our expert providers who specialize in treating Hypospadias:


