Read about upcoming changes to UnitedHealthcare coverage.
Immunotherapy has transformed cancer treatment over the past decade by boosting the body’s natural defenses to recognize and kill cancer. Immunotherapies work in a variety of different ways and have opened new doors for patients with cancers that were once very difficult to treat.
While cancer has evolved to evade the immune system in a number of ways, novel treatments and technologies are helping to overcome the ability of cancer to adapt and hide from the immune system. For example, drugs that turn off the brakes on the immune system are called immune checkpoint inhibitors. Therapies such as tumor-infiltrating lymphocyte (TIL) therapy expand a patient's own immune cells outside the body and then re-introduce them to the patient to increase the immune response. Chimeric antigen receptor (CAR) T-cell therapy, or engineered T-cell treatment, works by genetically modifying a patient’s own T-cells to recognize the tumor better.
Now, a newer approach called bispecific T-cell engager therapy, or BiTE therapy, is another powerful tool in the immunotherapy arsenal. Drs. Mateo Mejia, hematologist/oncologist at Weill Cornell Medicine, and Manish Shah, host of the CancerCast Podcast and Director of Solid Tumor Oncology at Weill Cornell Medicine, discuss this new therapy, including how it works, when it is used, and how safe it is.
T-cells are the immune system's primary weapon against disease. But when cancer develops, it finds ways to hide from T-cells or shut them down entirely. The result is an immune system that is present but not doing its job.
BiTE therapy addresses this directly. Rather than turning off the brakes or engineering new, modified T cells, it physically brings together T-cells and cancer cells by leveraging the two-arm structure of antibodies. While antibodies are already a part of the body’s immune system, natural antibodies can sometimes be ineffective in recruiting T-cells to directly fight the cancer. The antibodies used in BiTE therapy are developed in the lab to help the immune system with this process.
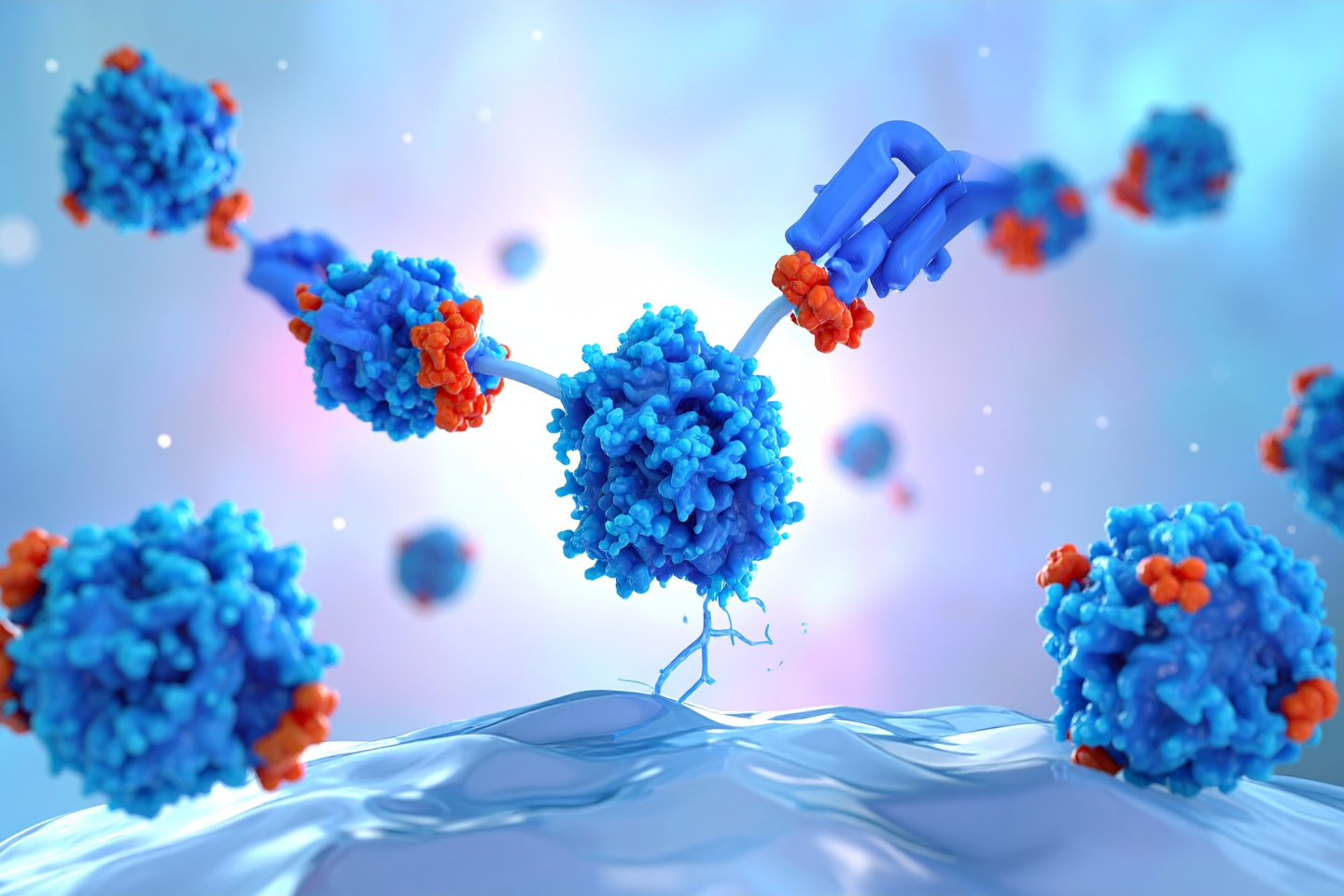
Dr. Manish Shah elaborates on what makes BiTEs unique. One arm of the BiTE molecule binds to a protein found on all T cells while the other arm binds to a protein on the cancer cell. “Instead of both arms attacking or binding to the same protein, they’re binding to different proteins, and the different proteins are on different cells,” he explains. The result is an immune response against the cancer that is able to help kill the cancerous cells.
Dr. Mateo Mejia explains it with an analogy. "Imagine it's like a person with two hands. The left hand grabs the T-cell that is not doing what it's supposed to and the right hand is going to grab the cancer cell,” he states. “By bringing them together, the T-cell gets activated and attacks the cancer."
BiTE therapy and CAR-T therapy, another cutting-edge immunotherapy, are like “cousins” since they share some similarities. Both aim to activate T-cells against cancer, but there are important differences. CAR-T therapy requires removing a patient's T-cells, engineering them in a lab to add a new T-cell receptor on the T-cell, and then reinfusing them back into the body, which can be a complex and time-intensive process. BiTE therapy, by contrast, is available “off-the-shelf” which means it is already premade and available for immediate use.
"These medications can be much more accessible to patients because we’re not modifying T-cells which takes time and an individual manufacturing process,” notes Dr. Mejia Saldarriaga. “Since there's no delay between the decision to treat and the start of treatment, this often makes BiTE therapy a better choice for patients who need treatment quickly.
BiTE therapy is given to patients via intravenous (IV) infusion or subcutaneous (under the skin) injection. Patients typically start at a lower dose that increases over time until they reach the recommended dose that is appropriate for their individual cancer. Treatment is usually given once every 1-2 weeks but could also be given less frequently after a positive response or after being on the therapy for an extended time period.
Patients are monitored closely by their healthcare team for any potential reactions, which may require a hospital stay or close outpatient follow-up at the start of treatment. After that, patients can typically go home the same day after BiTE treatment.
As with any therapy that activates the immune system, BiTE treatment can cause side effects. The two most important are cytokine release syndrome (CRS) and immune effector cell-associated neurotoxicity syndrome, or ICANS.
CRS occurs when the activated T-cells release large amounts of inflammatory proteins, causing symptoms such as fever, low blood pressure, and in more severe cases, effects on other organs. ICANS, involves that same inflammation affecting the brain, leading to symptoms such as confusion, headaches, or changes in cognitive function.
The good news is that both conditions are well understood and manageable. CRS most commonly occurs during the first doses of treatment, when more T-cells are being activated for the first time. As treatment continues, the risk decreases. ICANS, while potentially alarming, is typically short-lived and it usually resolves within one to five days.
While these side effects can indicate that a response to the treatment is happening, patients don’t need to experience these side effects for the therapy to be effective and having side effects also does not reduce the effectiveness of the therapy. Dr. Mejia emphasizes, "If you're not feeling well, we can treat the inflammation. It's going to make you feel better and we're not compromising in any way the efficacy of the treatment."
The immune system is set up in a way that once there is activation, more cells go to that area to try and kill off the cancer. If that isn’t kept in check, there could be an excess of inflammation, which is what may occur when BiTE therapy is first introduced into the body to activate the immune system.
“There’s a balance between activating and turning the immune system off,” Dr. Shah explains. “If you activate too much, you can get overstimulation of the immune system and that needs to be managed.”
Dr. Mejia uses a vivid analogy to explain the balance physicians are trying to strike. "We're going to create a little bit of fire. And that fire is good because it's going to kill the cancer, but we don't want to burn the whole house."
BiTE therapy is already Food and Drug Administration (FDA) approved for several cancers. In multiple myeloma alone, four different BiTE molecules are currently approved, targeting proteins called BCMA and GPRC5D which are highly expressed in myeloma cells. Beyond myeloma, BiTE therapy approvals exist for B-cell lymphomas, acute lymphoblastic leukemia, small cell lung cancer, and uveal melanoma—bringing the total to nearly ten approved BiTE therapies across different cancer types. Research is underway to explore how BiTE therapy may be useful in other solid tumor types, as well.
And, the field is moving fast which is very encouraging. Researchers are now exploring trispecific antibodies, which are molecules with not just two, but three arms targeting yet another protein on the cancer cell. Early data in heavily treated myeloma patients looks promising for the three-arm antibodies, and some of these newer molecules may actually be safer than their predecessors, even as they become more powerful.
There is also an exciting push to use these therapies earlier in the disease course. Current BiTEs are approved for patients that have been treated with multiple other therapy types, but clinical trials are now exploring BiTE therapy as a first-line treatment for newly diagnosed myeloma patients.
"We’re looking at earlier use of these immunotherapies, combinations to make it better, and new bispecific antibodies that are probably safer and even better than what we have already," Dr. Mejia says.
Dr. Shah frames the logic clearly. "If you have a target and you're able to hit the target well, the earlier in the disease course you utilize that target, the more effective your treatment's going to be," he offers.
These ongoing research efforts are looking at ways to best treat patients most effectively, while reducing toxicity and giving patients personalized treatment that is most applicable to their individual case.
To hear more from Drs. Mejia and Shah on bispecific antibodies, tune in to the Weill Cornell Medicine CancerCast podcast where they dive into more specifics about this form of treatment. Listen to this episode on Apple Podcasts, Spotify, YouTube or the Weill Cornell Medicine website.